

Background
HLA-haploidentical (haplo) blood or marrow transplantation (BMT) with post-transplantation cyclophosphamide (PTCy) is widely used, but few factors that inform donor selection have been identified. Based on prior observations for HLA-B leader (EW Petersdorf et al. Lancet Haematol 2020), HLA-DRB1 (YL Kasamon et al. BBMT 2010), and HLA-DPB1 (SR Solomon et al. BBMT 2018), we hypothesized that mismatching at individual HLA loci may influence BMT outcomes, but single and additive HLA gene effects have not been evaluated systematically in the context of haploBMT with PTCy.
Methods
The Center for International Blood and Marrow Transplant Research (CIBMTR) identified 1,434 patients who underwent T-cell-replete haploBMT with PTCy for acute leukemia or myelodysplastic syndrome (MDS) between 2008-2017. Multivariable models assessed transplant outcomes associated with 3 HLA-factors: (1) B-leader dimorphism (MM, MT, TT) matching; (2) HLA-DRB1 mismatching in the graft-versus-host (GVH) direction; and (3) nonpermissive HLA-DPB1 mismatching in the GVH direction using the T-cell epitope-3 model, which classifies HLA-DPB1 mismatches into permissive or non-permissive. All final models contained the HLA factors and adjusted for other significant clinical covariates at p<.05 in univariate analysis. P-values were not adjusted for multiple testing.
Results
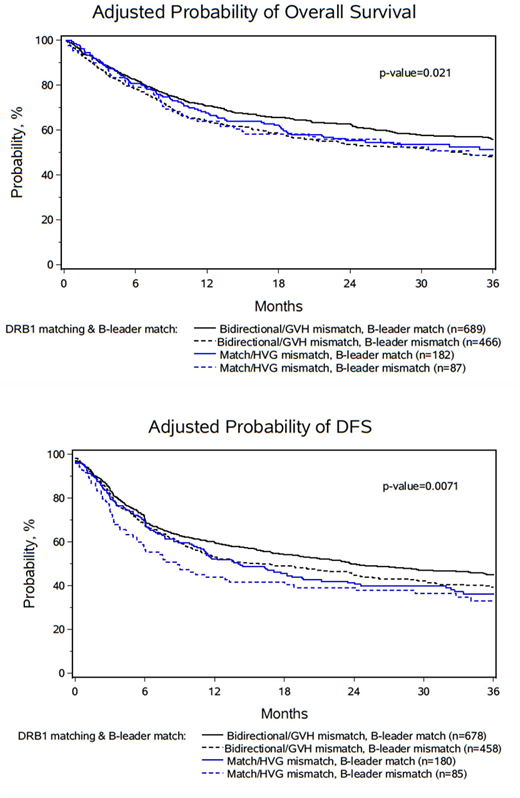
Diagnoses were 58% AML, 23% ALL, 19% MDS. 22% of AML patients were in advanced disease stage (relevant analyses were stratified for disease stage for both acute leukemia and MDS). Median recipient age was 54 (range 1-78) years. Median follow up among survivors was 12 (range 2-119) months. Marrow was the graft source in 43% of recipients. Myeloablative conditioning was used in 45% of recipients. Fifty percent of recipients had hematopoietic cell transplantation-comorbidity index (HCT-CI) scores of ≥3. HLA-DP typing was missing in 52% of cases and thus all models had a "missing" category for HLA-DP. Mismatching in the GVH direction at HLA-A, HLA-C, or HLA-DQ was not associated with study outcomes [overall survival (OS), disease-free survival (DFS), relapse, nonrelapse mortality (NRM), or grade II-IV acute, grade III-IV acute, or chronic graft-versus-host disease (gr2-4a or cGVHD)]. When compared to leader-matched patients, HLA-B leader-mismatching was associated with worse OS and DFS (hazard ratio [HR] 1.25 [95% CI, 1.09 to 1.44]; P=.002, and HR 1.18 [95% CI, 1.03 to 1.34]; P=.01, respectively), and higher risk of NRM (HR 1.38 [95% CI, 1.10 to 1.74]; P=.005), but was not associated gr2-4a or cGVHD, or relapse. In contrast, when compared to matching at HLA-DRB1, the presence of any GVH direction mismatch at HLA-DRB1 was associated with improved DFS (HR 0.80 [95% CI, 0.68 to 0.94]; P=.007) and lower risk of relapse (HR 0.69 [95% CI, 0.56 to 0.86]; P=.0008), but with no effect on OS, gr2-4a or cGVHD, or NRM. Similarly, any nonpermissive GVH mismatching at HLA-DPB1 was also associated with improved DFS (HR 0.72 [95% CI, 0.55-0.94], p=.015) and OS (HR 0.59 [95% CI, 0.43-0.82], p=.002), with a tendency towards lower relapse (HR 0.75 [95% CI, 0.54-1.05], p=.09), but with no effect on gr2-4a or cGVHD, or NRM. When combining the effects of leader matching at HLA-B and mismatching at HLA-DRB1 there was an additive improvement in both DFS and OS (Figure 1 A and B) with significantly lower NRM (p=0.03) and relapse (p=0.008) when compared to other groups. Within this unselected large cohort, favorable haplo donors based on B-leader matching and HLA-DRB1 mismatching were used for 48.5% of recipients and had improved DFS (HR 0.68 [95% CI, 0.52 to 0.88], p=.004) when compared to B-leader mismatched and HLA-DRB1 matched pairs, suggesting that with intentional selection of donors based on these factors, even more could receive a favorable combination.
Conclusion
HLA-B leader mismatching is a risk factor for NRM and worse OS and DFS, whereas either HLA-DRB1 or nonpermissive HLA-DPB1 mismatch is associated with reduced relapse and improved DFS, after haploBMT with PTCy. PTCy dissociates the graft-versus-leukemia effect of HLA-DRB1 and nonpermissive HLA-DPB1 mismatching from GVHD. The best outcomes after haploBMT with PTCy are seen when a donor is HLA-B leader matched and HLA-DRB1 mismatched. When there is more than one potential haplo donor for an acute leukemia or MDS patient, selection based on HLA considerations may improve DFS and OS.
Shaw:Orca Bio: Consultancy. Lee:Takeda: Research Funding; AstraZeneca: Research Funding; Novartis: Research Funding; Incyte: Consultancy, Research Funding; Syndax: Research Funding; Pfizer: Consultancy, Research Funding; Amgen: Research Funding; Kadmon: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal